Understanding Osteoporosis in Seniors
Symptoms and Diagnosis of Osteoporosis
Recognizing the Early Signs
Osteoporosis, often referred to as the silent thief, progressively weakens bones, leaving them fragile and susceptible to fractures. Early symptoms tend to be subtle and frequently go unnoticed, especially among older adults. Since pain or discomfort may not manifest initially, understanding risk factors and scheduling routine medical evaluations becomes paramount. While some people report noticeable bone pain, many others don’t, highlighting the critical need for proactive screening.
Subtle indicators like persistent back pain, gradual height loss, or a stooped posture often get dismissed as normal aging. However, any ongoing or worsening back discomfort warrants a doctor’s visit. A detailed medical history and physical exam can uncover potential issues and guide further diagnostic steps.
Diagnostic Tests and Procedures
Diagnosing osteoporosis requires a multifaceted approach to evaluate bone density and strength. The gold standard is the dual-energy X-ray absorptiometry (DEXA) scan, a non-invasive test measuring bone mineral density (BMD) at key sites like the hip and spine. DEXA results provide quantifiable data, enabling comparisons to normative values and assessing bone loss severity.
Additional tools, such as blood tests for calcium and vitamin D levels, help identify deficiencies impacting bone health. In complex cases, bone biopsies might be used to examine microarchitecture and composition more closely.
Factors Influencing Diagnosis
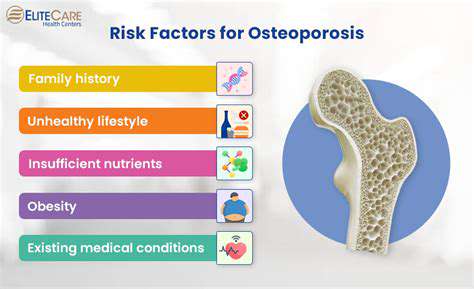
Accurate osteoporosis diagnosis extends beyond bone density metrics. A patient’s medical history—previous fractures, family osteoporosis cases, and current medications—plays a pivotal role. Lifestyle factors, including diet, physical activity, and smoking, also shape the assessment. For instance, inadequate calcium/vitamin D intake or smoking can severely compromise bone density.
Demographics like age, gender, and ethnicity further refine risk stratification. Post-menopausal women face higher osteoporosis risks, as do certain ethnic groups. Chronic conditions (e.g., hyperthyroidism or celiac disease) may also contribute to bone loss, necessitating thorough medical history reviews.
Importance of Early Intervention
Early detection is vital for managing osteoporosis and preventing fractures, which can cause chronic pain, mobility loss, and diminished quality of life. Timely interventions—lifestyle changes, dietary adjustments, and medications—can slow bone deterioration. Regular follow-ups ensure treatment efficacy and allow for timely adjustments.
Medications and Therapies for Osteoporosis
Pharmacological Treatments for Osteoporosis
Bisphosphonates (e.g., alendronate, risedronate) are first-line treatments, inhibiting bone resorption. Patients must follow administration guidelines—taking the drug with water and staying upright—to avoid esophageal irritation. Denosumab, an injectable, targets bone-breakdown cells and requires periodic dosing. Treatment choices should balance benefits, side effects, and individual health profiles.
Hormone Replacement Therapy (HRT)
HRT can preserve bone density in post-menopausal women by replenishing estrogen. However, risks like blood clots and certain cancers necessitate careful risk-benefit discussions with a healthcare provider.
Selective Estrogen Receptor Modulators (SERMs)
SERMs like raloxifene mimic estrogen’s bone-protective effects but may cause hot flashes or clotting issues. These trade-offs must be weighed against therapeutic gains.
Calcium and Vitamin D Supplements
Calcium and vitamin D are foundational for bone health, but excessive supplementation can backfire. Dietary sources are ideal, though supplements may be needed for seniors. Dosages should be medically supervised.
Lifestyle Modifications
Weight-bearing exercise, calcium/vitamin D-rich diets, and avoiding smoking/alcohol are cornerstones of osteoporosis management. Activities like walking enhance bone strength and balance, reducing fall risks.
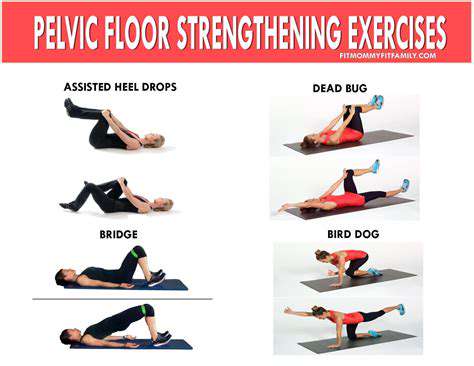
Physical Therapy and Fall Prevention Strategies
Customized physical therapy programs improve strength and coordination, mitigating fall risks. Home safety tips—removing tripping hazards, improving lighting—further safeguard against fractures.
Alternative Therapies
Herbal remedies or acupuncture lack robust evidence for osteoporosis. Consult a doctor before trying alternatives to avoid drug interactions or adverse effects.
Read more about Understanding Osteoporosis in Seniors

![Best Meditation Apps for Beginners [2025 Review]](/static/images/26/2025-05/Top3MeditationAppsforBeginnersin2025.jpg)

![Best Books on Mental Health and Well being [Recommended Reads]](/static/images/26/2025-05/CultivatingSelf-CompassionandPositiveSelf-Talk.jpg)



Hot Recommendations
-
*Guide to Managing Gout Through Diet
-
*Best Habits for Financial Well being
-
*How to Build a Routine for Better Mental Health
-
*How to Eat Healthy on a Budget [Tips & Meal Ideas]
-
*Guide to Practicing Self Acceptance
-
*How to Incorporate More Movement Into Your Day
-
*Guide to Managing Chronic Pain Naturally
-
*Guide to Building a Reading Habit for Well being
-
*Top 5 Weight Loss Supplements That Actually Work
-
*Best Exercises for Postpartum Recovery [Beyond Abdominal Work]